
When Medications Quiet More Than Hunger
She came back to me a few weeks after our first conversation and said something I've been thinking about since.
"The medication is working," she told me. "The labs look better. I'm not thinking about food all day. But Friday doesn't feel like Friday anymore."
What she meant was that the wine she'd always used to close out her work week had lost its pull. The Sunday cooking she used to look forward to, the ritual of it, the way it anchored her family and let her express something she didn't always say in words, had become something to get through. Her husband would say something at dinner and she'd realize she'd been somewhere else.
She was relieved about her health. She was unsettled about almost everything else.
Recently, Canadian Affairs published a piece by journalist Alexandra Keeler that gave what she was experiencing a name. The article includes one of my members at The Shift Clinic and several physicians, including me. It captures something the field has been slow to talk about: that the medications working so well on weight are quieting other parts of patients' lives, and that quieting isn't free.
The volume knob problem
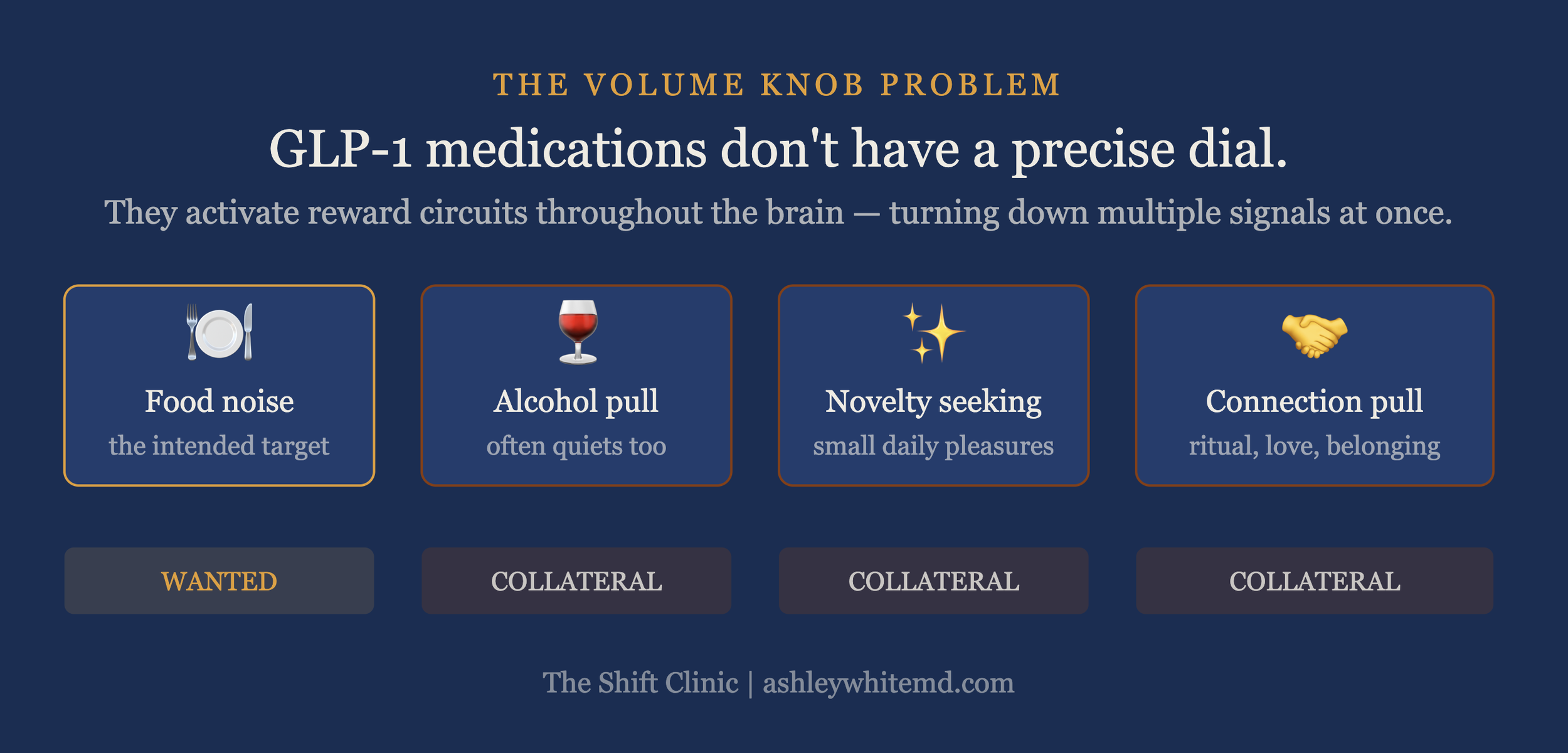
GLP-1 receptors don't live only in the gut. They sit in the brain's reward circuitry, the same regions where dopamine signaling drives the pull toward food, alcohol, novelty, and the people we love.
When these medications activate those receptors, the pull is dampened broadly. Food noise quiets. Sometimes so does the desire for alcohol, the impulse to shop, or the small daily stimulations that used to register as pleasure. Dr. Peter Lin, a Toronto physician quoted in the same piece, described GLP-1 medications as something more like a volume knob on a stereo than a precise dial. They turn everything down at once.
What I told the reporter is that these medications are a blunt instrument. That's not a criticism. It's a description of what they are. Anything the brain has learned to experience as pleasure can be turned down by them, which is the same property that makes them effective for weight, for alcohol use disorder, and for the intrusive food thoughts that have dominated my patients' inner lives for decades.
We may eventually have GLP-1 medications with separate dials for food and the rest of life. We don't have them yet.
What I want patients to keep, while the medication does its work on hunger, is what makes a life worth living: the capacity to fall in love, the pull toward the people they want at their table, the lift of hearing music that means something. Treatment has to be designed around protecting those things, even as the research on isolated reward dampening continues to develop.
What food was actually doing
The blunting matters most because for most of the women I see, food has not been only fuel for a long time.
It's been what makes Friday different from Wednesday. How a hard day becomes survivable. Where connection happens around a table. Some of that they are glad to renegotiate: the part where eating felt compulsive, where the wanting was loud all day, where they couldn't sit through a meeting without thinking about what they'd eat afterward. That kind of relief is real and significant.
The rest is harder. The wine that closed the work week. The cooking that anchored the family. The small pleasure of a meal eaten slowly with people they love. Those don't belong in the same category as food noise. Both relief and loss can show up in the same patient in the same week, and both are telling the truth.
There's a second piece, more clinical, that I want to name here. For many of these patients, food has also been a regulator. A way to come down from a hard meeting. To bridge a lonely evening. To soften the edges of an argument before bed. When the medication blunts food's reward, it also blunts the muting effect food had on negative emotion. Patients often describe feeling the lows more clearly while the highs sit at lower volume.
For patients with histories of trauma or substance use, where food has been a coping mechanism keeping worse coping mechanisms at bay, this can be destabilizing. It deserves a conversation before the first injection, not a discovery a few months in.
If you want to understand your own appetite patterns, including what your hunger signals have been carrying, theShift Strategy Quiz is a good starting point. It takes about five minutes and helps surface what might be worth talking to a clinician about before you start.
What good prescribing actually requires
None of this is a reason to stop GLP-1 treatment. The pharmacology is doing real clinical work on insulin signaling, gastric emptying, and satiety. For many patients, the relief from decades of relentless food preoccupation is genuinely life-changing. These medications belong in the toolkit of modern obesity care.
The question is not whether they should be prescribed. It's what kind of clinical relationship has to surround the prescription for a patient to do well over years, not just months.
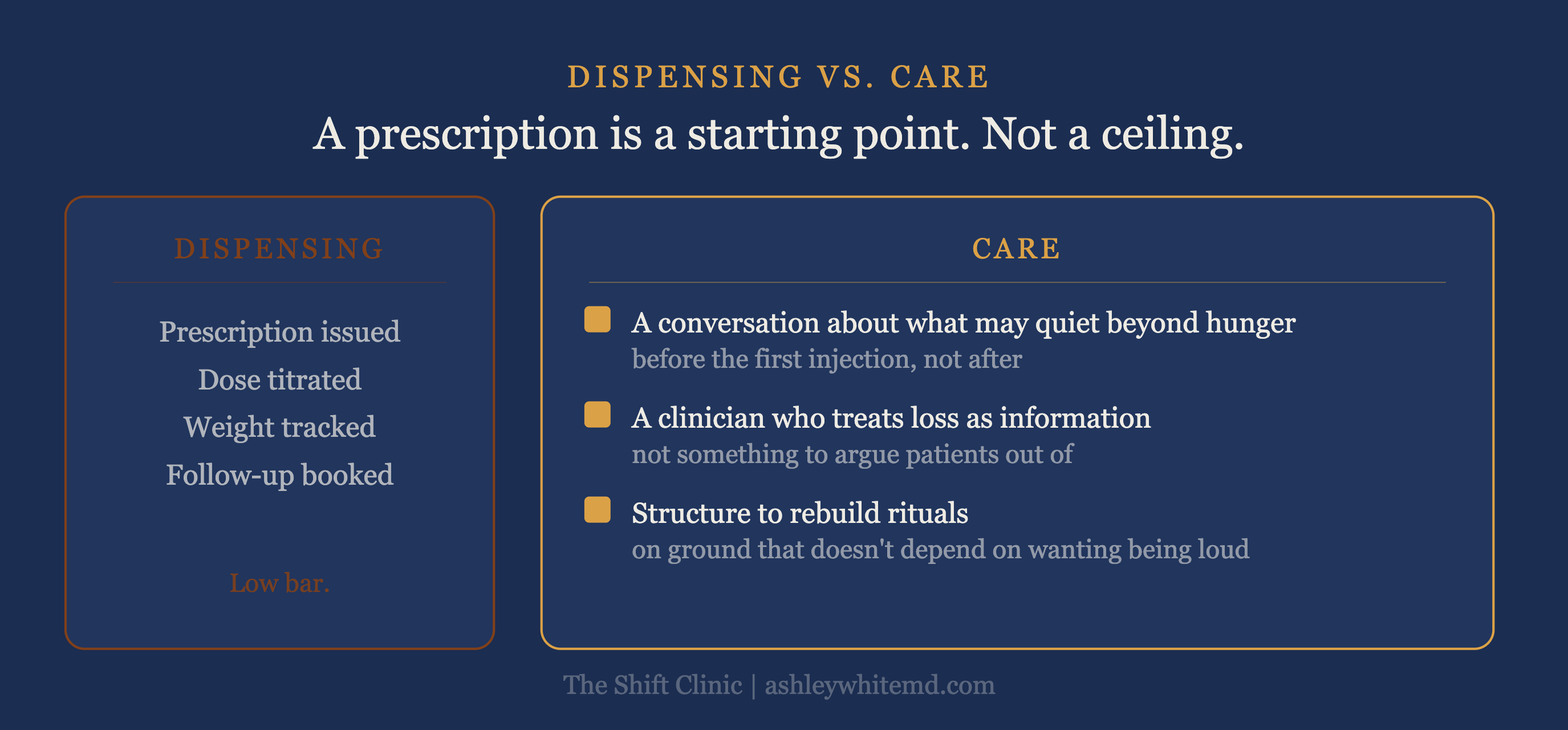
Beyond thoughtful dosing and continuous feedback, which is a starting point and not a ceiling, patients actually need several things the field has been slow to offer. A conversation that names what may quiet beyond hunger before the first injection, not after. A clinician who can tell the difference between a meaningful loss and a transient adjustment, and who treats the loss as information rather than something to argue them out of. Time and structure to rebuild rituals on ground that doesn't depend on wanting being loud.
A prescribing relationship that skips that work is dispensing, not care.
The patients who do best on these medications are not the ones who feel only gratitude for the weight loss. They're the ones who let themselves notice both the relief and the loss, and who get help making sense of what the medication has changed about how their life feels from the inside.
Rebuilding what matters
The patient I described at the start came back to me weeks after that first difficult conversation. She had started noticing what Friday used to do for her: that the wine had been a small ritual closing the work week, that the cooking had been how she expressed care for her family. Both had quieted enough that she'd begun to grieve a version of her life she hadn't realized she was living inside.
None of that, she was clear, made her want to stop the medication. It made her want better help making sense of what it had changed.
That framing is exactly right. The goal isn't to preserve the coping mechanism. The goal is to understand what the coping mechanism was carrying, and then to build something more durable in its place. Rituals that don't depend on reward circuitry being loud. Connection that doesn't require a particular glass of wine to unlock. A Friday that has its own shape.
This is perspective work, in the language of the MAP Framework I use with every patient. Metabolism and appetite are only two of the three domains. Perspective, how you see yourself, how you navigate change, how you make sense of what's shifting, is where the long-term work lives.
GLP-1 medications create metabolic space. What you put in that space determines whether this time is different.
If this is you
If you're on a GLP-1 medication and you recognize some of what I've described, the flattening, the Friday that doesn't feel like Friday, the quieted pull toward people or pleasures that used to organize your week, you are not malfunctioning. You are paying attention.
That noticing is the beginning of good care, not the end of it. The work is to take what the medication is offering and rebuild the rest of your life around the changes it has made, with clinicians who can hold both the relief and the loss in the same room.
Membership at The Shift Clinic is built for women who want their GLP-1 care to include that second conversation: not only the prescription, but the ongoing clinical relationship that makes the prescription worth something. If you're already on medication through another provider and want to add that layer of support, you can maintain or switch your care here.
This is what obesity medicine looks like when it's done well: not a prescription handed across a desk, but a framework for understanding what's changing, what to hold onto, and how to build something that lasts.