
Are We All Just Quitters? Issues with staying on weight loss treatment aren’t going away.

A patient messaged me last month after reading about discontinuation rates for GLP-1 medications. “Wait,” she wrote. “That many people stop? Even when the medication is free?”
It’s a fair question. And the answer is yes.
A 2025 study published in JAMA followed 125,474 adults who started GLP-1 treatment across US healthcare systems. For people taking these medications for obesity (not diabetes), nearly two-thirds had stopped within one year. By two years, that number was 84.4%.
If you’re taking semaglutide or tirzepatide for weight management, you are statistically in the minority if you’re still on it two years later. And the question worth asking isn’t “what’s wrong with the people who quit?” It’s “what’s missing from most of these treatment models?”
The numbers
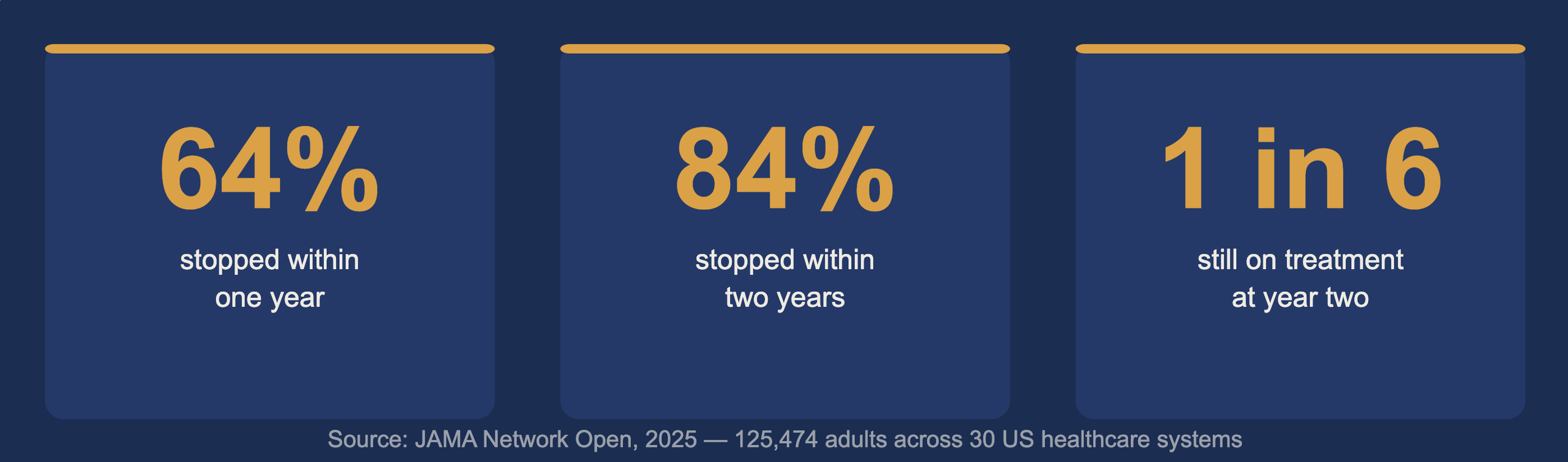
The JAMA Network Open study is the most rigorous real-world data we have on this. Researchers analyzed electronic health records from 30 US healthcare systems over five years. Overall, more than half of all GLP-1 users had stopped within twelve months. Among people without diabetes taking the medication specifically for obesity, discontinuation hit 84.4% by year two.
Here’s what stood out to me: the strongest predictor of staying in treatment was simply seeing results. Patients who were losing weight stayed. Patients who weren’t, left.
That sounds obvious. But it points to something important. The people who stopped weren’t quitters. They were running on fumes: no support when side effects hit, no one to call when things got complicated, no framework to return to when the early momentum flattened out.
The hardware problem
This makes me think of Peloton. Bear with me. I promise this is relevant.
The company bet everything on the bike. If people had the hardware, they’d use it. They nearly went bankrupt because they had it backwards. The bike was not the product. The subscription was. The community, the coaching, the accountability: that was what people were actually buying. The bike was just how it got delivered.
GLP-1 medications are the bike
When medication is the entire offering, a prescription, a refill reminder, maybe a quarterly check-in, you have hardware with no subscription. A tool with no system around it. And tools without systems produce early results, then confusion, then dropout.
The patients who stop are not failing the medication. They are being failed by a model that assumed the medication was enough.
What actually keeps people in treatment
If it’s not cost and it’s not willpower, what predicts persistence?
Support structures. Specifically: an ongoing physician relationship, real education about what’s happening in your body, community with others navigating the same experience, and a framework to return to when things stop being simple.
When we asked members of The Shift Clinic what they’d be most upset to lose, the top answer wasn’t their prescription. It was direct access to their physician. The relationship came first. The medication followed.
Members describe it as waiting years for this kind of care and finally finding it. Not because of the drug alone. Because someone was holding the whole picture, metabolic, psychological, practical, and helping them navigate it.
The research backs this up. The strongest predictor of staying in treatment is feeling genuinely understood by your care team. Not just managed. Not just refilled. Understood.
That’s a different bar than most treatment models are built to meet.
What real support looks like
Here’s what happens when appetite suppression is the whole plan: it works, until it doesn’t.
In the early months on a GLP-1, the suppression can feel almost effortless. Food noise quiets. Portions naturally decrease. Weight starts to move. Then something shifts. The suppression plateaus. A stressful stretch hits. Side effects get complicated. The medication needs adjusting. And if no one has ever explained why your body is doing what it’s doing, you have nothing to stand on.
Patients who understand their physiology don’t panic when results aren’t linear. They know that appetite regulation isn’t the same as appetite elimination. They know that hunger signals change over time on medication, and that this is expected. They know the difference between a headwind that needs addressing and a sign that treatment has failed.
A prescription doesn’t teach you that. A system does.
This is why the work at The Shift Clinic is built around what we call Appetite Literacy: the foundational skill of learning to read your body’s signals accurately. Not suppressing them. Not overriding them. Actually understanding what they mean. A patient who’s developed real appetite literacy doesn’t need the medication to do all the work. She brings knowledge into the equation. And that knowledge persists when circumstances change.
It also means having somewhere real to bring the hard weeks. Our community is professionally moderated and physician-present. Members are working from the same framework, which means they share what’s actually happening without the toxic comparison that derails most weight-related groups. Sixty percent of active members engage weekly, not because they’re required to, but because it genuinely helps.
And it means ongoing skill-building that goes beyond how the medication works. We work across three areas: the identity and psychological layer, appetite literacy and practical metabolic skills, and strategic planning that connects what you care about to what you actually do. Not as lectures. As working sessions, month after month.
None of this is separate from the clinical care. The education informs medication decisions. Community conversations show up in physician appointments. Strategy sessions shape how members approach the hard months. It’s one system.
The MAP Framework
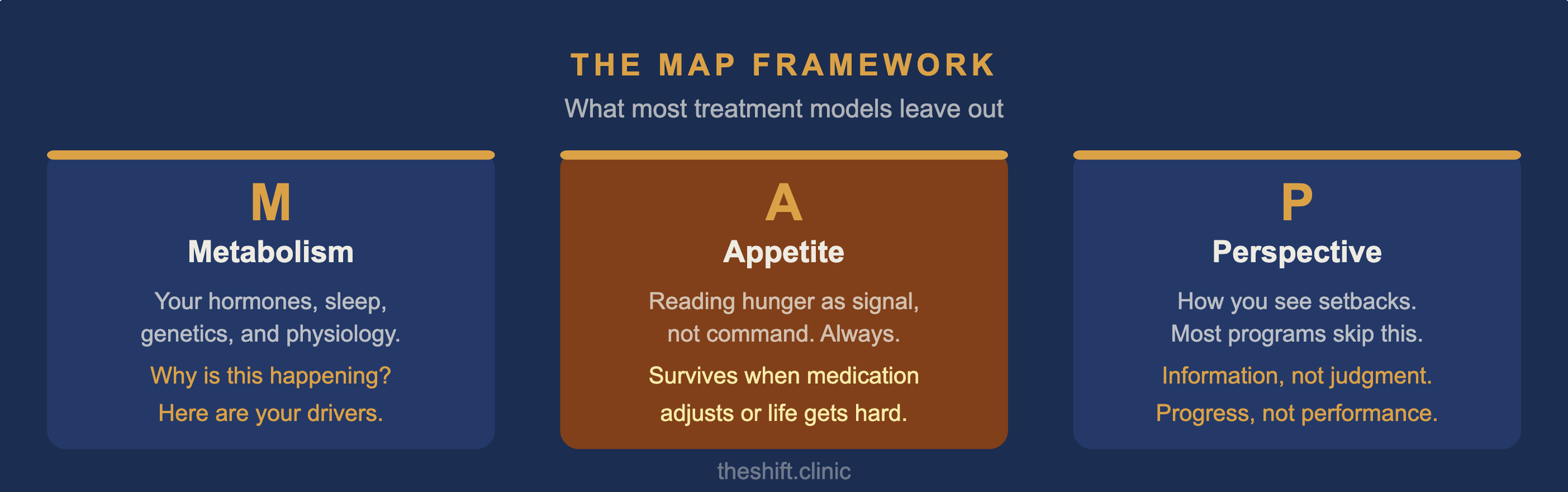
Beneath all of it sits our MAP Framework: Metabolism, Appetite, Perspective.
Most treatment models address one of these, maybe two. They handle the metabolic piece: medication and perhaps some dietary guidance. Then they hope the rest follows. It usually doesn’t.
Metabolism matters because understanding your specific physiology, your hormonal patterns, your sleep, conditions like PCOS or insulin resistance, changes the conversation from “why isn’t this working?” to “here are my specific drivers, and here’s how we address them.”
Appetite matters because learning to read hunger as a signal rather than a command is the skill that survives when medication adjusts, when life gets complicated, when you travel or sleep poorly or go through a hard stretch. Appetite literacy doesn’t depend on perfect conditions.
Perspective is the layer most programs skip entirely, and it’s often what kills persistence. How do you see yourself? How do you navigate setbacks? Whether you treat a difficult week as evidence of failure or as information about what needs adjusting, that determines everything. The patients who stay in treatment aren’t the ones who never struggle. They’re the ones who’ve built a different relationship with struggle. This time can be different
The 85 percent dropout rate is not a statement about patient commitment. It is a statement about what most treatment models are missing.
When someone stops a GLP-1 medication at month four, the analysis is not that she lacked willpower. The analysis is that the support infrastructure was not there. No one explained what to do when appetite suppression changed. No one was available when things got complicated. No community normalized the experience. No framework survived the hard weeks.
The medication creates space. What surrounds it determines whether that space becomes something lasting.
If you are ready to find out what comprehensive GLP-1 care actually looks like, The Shift Clinic was built around that question. If you want to understand your own patterns first, The Shift Quiz is a good place to start. And if you want to understand how this practice came to exist, the origin story is worth reading.